
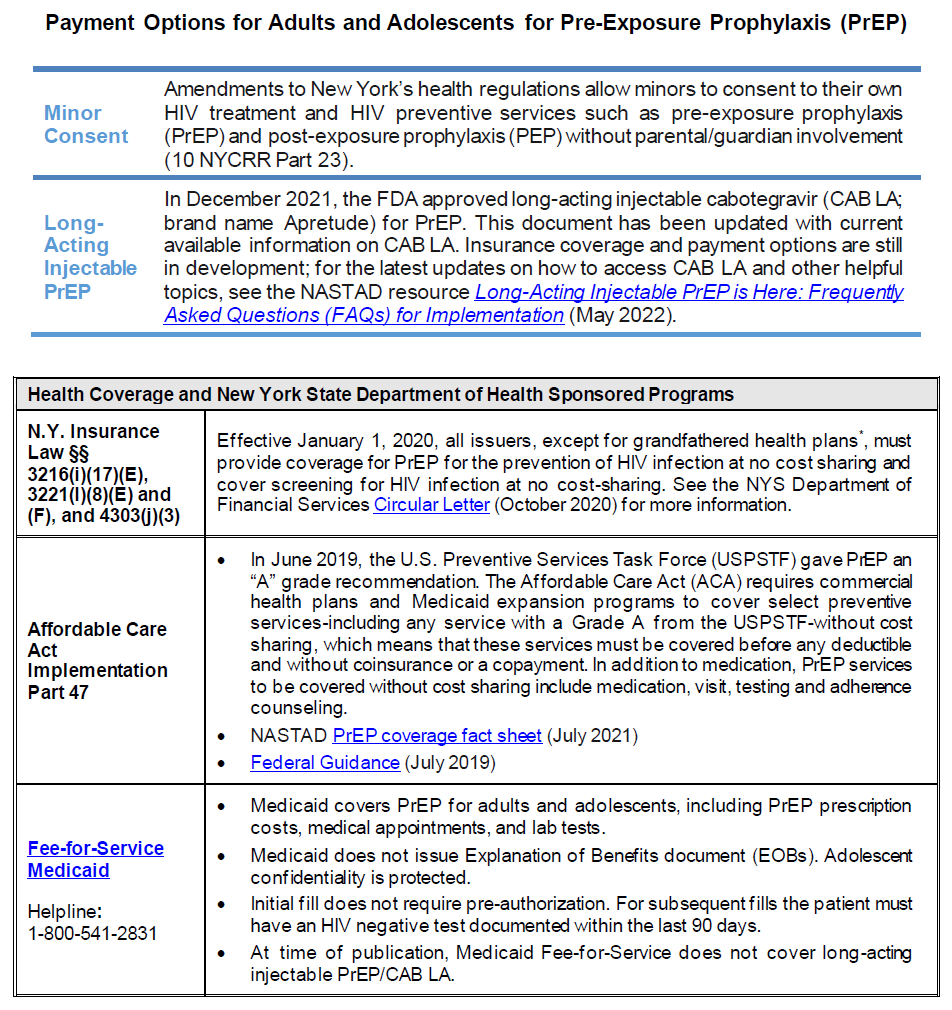
PrEP Payment Options
Click the image below to download a PDF from www.health.ny.gov
Online Resources for Education, Information, and Services
June 2022
This section contains additional resources for care providers, including information, services, tools, and laws, about or related to HIV pre-exposure prophylaxis (PrEP).
New York State Department of Health:
- Beyond Status
- What Support Services Providers Should Know About HIV Clinical Guidelines: PrEP to Prevent HIV and Promote Sexual Health
- Medicaid Coverage for HIV PrEP-Related Services
- Truvada and Descovy Medicaid Fee-for-Service
- PrEP Information for Clinicians
- PrEP Provider Directory
- PrEP for Sex
- Uninsured Care Programs
- Sexually Transmitted Infections (STIs) Information for Providers
- STI Self-Collection Outside of a Clinic Setting in New York State (NYS) Question & Answer
- Communicable Disease Reporting
- HIV/AIDS Laws & Regulations
- What Health Care Providers Need to Know About Partner Services
- Clinical Education Initiative (CEI): HIV Primary Care and Prevention, Sexual Health, HCV Treatment, and Drug User Health
- CEI: PrEP/PEP Resources
- CEI: PrEP Clinical Cards
New York City Health:
NASTAD: PrEP Coverage Brief: PrEP Services Covered With No Cost Sharing
Centers for Disease Control and Prevention: PrEP Resources for Care Providers
Clinicalinfo.HIV.gov: Drug Database
HIV-ASSIST: Free Clinical Decision-Making Support for ARV Selection
PleasePrEPme.org: Provider Resources
University of California San Francisco: Pre-Exposure Prophylaxis Phone Consultation
University of Liverpool: HIV Drug Interactions
GOALS Framework for Sexual History Taking in Primary Care
Download Printable PDF of GOALS Framework
Developed by Sarit A. Golub, PhD, MPH, Hunter College and Graduate Center, City University of New York, in collaboration with the NYC Department of Health and Mental Hygiene, Bureau of HIV, July 2019
Background: Sexual history taking can be an onerous and awkward task that does not always provide accurate or useful information for patient care. Standard risk assessment questions (e.g., How many partners have you had sex within the last 6 months?; How many times did you have receptive anal sex with a man when he did not use a condom?) may be alienating to patients, discourage honest disclosure, and communicate that the number of partners or acts is the only component of sexual risk and health.
In contrast, the GOALS framework is designed to streamline sexual history conversations and elicit information most useful for identifying an appropriate clinical course of action.
The GOALS framework was developed in response to 4 key findings from the sexual health research literature:
- Universal HIV/STI screening and biomedical prevention education is more beneficial and cost-effective than risk-based screening [Wimberly, et al. 2006; Hoots, et al. 2016; Owusu-Edusei, et al. 2016; Hull, et al. 2017; Lancki, et al. 2018].
- Emphasizing benefits—rather than risks—is more successful in motivating patients toward prevention and care behavior [Weinstein and Klein 1995; Schuz, et al. 2013; Sheeran, et al. 2014].
- Positive interactions with healthcare providers promote engagement in prevention and care [Bakken, et al. 2000; Alexander, et al. 2012; Flickinger, et al. 2013].
- Patients want their healthcare providers to talk with them about sexual health [Marwick 1999; Ryan, et al. 2018].
Rather than seeing sexual history taking as a means to an end, the GOALS framework considers the sexual history taking process as an intervention that will:
- Increase rates of routine HIV/STI screening;
- Increase rates of universal biomedical prevention and contraceptive education;
- Increase patients’ motivation for and commitment to sexual health behavior; and
- Enhance the patient-care provider relationship, making it a lever for sexual health specifically and overall health and wellness in general.
The GOALS framework includes 5 steps:
- Give a preamble that emphasizes sexual health. The healthcare provider briefly introduces the sexual history in a way that de-emphasizes a focus on risk, normalizes sexuality as part of routine healthcare, and opens the door for the patient’s questions.
- Offer opt-out HIV/STI testing and information. The healthcare provider tells the patient that they test everyone for HIV and STIs, normalizing both testing and HIV and STI concerns.
- Ask an open-ended question. The healthcare provider starts the sexual history taking with an open-ended question that allows them to identify the aspects of sexual health that are most important to the patient, while allowing them to hear (and then mirror) the language that the patient uses to describe their body, partner(s), and sexual behaviors.
- Listen for relevant information and fill in the blanks. The healthcare provider asks more pointed questions to elicit information that might be needed for clinical decision-making (e.g., 3-site versus genital-only testing), but these questions are restricted to specific, necessary information. For instance, if a patient has already disclosed that he is a gay man with more than 1 partner, there is no need to ask about the total number of partners or their HIV status in order to recommend STI/HIV testing and PrEP education.
- Suggest a course of action. Consistent with opt-out testing, the healthcare provider offers all patients HIV testing, 3-site STI testing, PrEP education, and contraceptive counseling, unless any of this testing is specifically contraindicated by the sexual history. Rather than focusing on any risk behaviors the patient may be engaging in, this step focuses specifically on the benefits of engaging in prevention behaviors, such as exerting greater control over one’s sex life and sexual health and decreasing anxiety about potential transmission.
Resources for implementation:
- Script, rationale, and goals: Box 1, below, provides a suggested script for each step in the GOALS framework, along with the specific rationale for that step and the goal it is designed to accomplish.
- The 5Ps model for sexual history-taking (CDC): Note that the GOALS framework is not designed to completely replace the 5Ps model (partners, practices, protection from STI, past history of STI, prevention of pregnancy); instead, it provides a framework for identifying information related to the 5Ps that improves patient-care provider communication, reduces the likelihood of bias or missed opportunities, and enhances patients’ motivation for prevention and sexual health behavior.
Download Box 1: GOALS Framework for the Sexual History Printable PDF
| Box 1: GOALS Framework for the Sexual History |
||
| Component | Suggested Script | Rationale and Goal Accomplished |
| Give a preamble that emphasizes sexual health. | I’d like to talk with you for a couple of minutes about your sexuality and sexual health. I talk to all of my patients about sexual health, because it’s such an important part of overall health. Some of my patients have questions or concerns about their sexual health, so I want to make sure I understand what your questions or concerns might be and provide whatever information or other help you might need. |
|
| Offer opt-out HIV/STI testing and information. | First, I like to test all my patients for HIV and other sexually transmitted infections. Do you have any concerns about that? |
|
| Ask an open-ended question. | Pick one (or use an open-ended question that you prefer):
|
|
| Listen for relevant information and probe to fill in the blanks. |
|
|
| Suggest a course of action. |
|
|
References
Alexander JA, Hearld LR, Mittler JN, et al. Patient-physician role relationships and patient activation among individuals with chronic illness. Health Serv Res 2012;47(3 Pt 1):1201-1223. [PMID: 22098418]
Bakken S, Holzemer WL, Brown MA, et al. Relationships between perception of engagement with health care provider and demographic characteristics, health status, and adherence to therapeutic regimen in persons with HIV/AIDS. AIDS Patient Care STDS 2000;14(4):189-197. [PMID: 10806637]
Flickinger TE, Saha S, Moore RD, et al. Higher quality communication and relationships are associated with improved patient engagement in HIV care. J Acquir Immune Defic Syndr 2013;63(3):362-366. [PMID: 23591637]
Hoots BE, Finlayson T, Nerlander L, et al. Willingness to take, use of, and indications for pre-exposure prophylaxis among men who have sex with men-20 US cities, 2014. Clin Infect Dis 2016;63(5):672-677. [PMID: 27282710]
Hull S, Kelley S, Clarke JL. Sexually transmitted infections: Compelling case for an improved screening strategy. Popul Health Manag 2017;20(S1):S1-s11. [PMID: 28920768]
Lancki N, Almirol E, Alon L, et al. Preexposure prophylaxis guidelines have low sensitivity for identifying seroconverters in a sample of young Black MSM in Chicago. Aids 2018;32(3):383-392. [PMID: 29194116]
Marwick C. Survey says patients expect little physician help on sex. Jama 1999;281(23):2173-2174. [PMID: 10376552]
Owusu-Edusei K, Jr., Hoover KW, Gift TL. Cost-effectiveness of opt-out chlamydia testing for high-risk young women in the U.S. Am J Prev Med 2016;51(2):216-224. [PMID: 26952078]
Ryan KL, Arbuckle-Bernstein V, Smith G, et al. Let’s talk about sex: A survey of patients’ preferences when addressing sexual health concerns in a family medicine residency program office. PRiMER 2018;2:23. [PMID: 32818195]
Schüz N, Schüz B, Eid M. When risk communication backfires: randomized controlled trial on self-affirmation and reactance to personalized risk feedback in high-risk individuals. Health Psychol 2013;32(5):561-570. [PMID: 23646839]
Sheeran P, Harris PR, Epton T. Does heightening risk appraisals change people’s intentions and behavior? A meta-analysis of experimental studies. Psychol Bull 2014;140(2):511-543. [PMID: 23731175]
Weinstein ND, Klein WM. Resistance of personal risk perceptions to debiasing interventions. Health Psychol 1995;14(2):132-140. [PMID: 7789348]
Wimberly YH, Hogben M, Moore-Ruffin J, et al. Sexual history-taking among primary care physicians. J Natl Med Assoc 2006;98(12):1924-1929. [PMID: 17225835]


